BRAIN ANEURYSMS
How does a Hemorrhagic stoke or Brain bleed occur?
What is a Brain aneurysm? What are the risk factors for aneurysm rupture?
What is a Brain aneurysm? What are the risk factors for aneurysm rupture?

Bleeding in the brain occurs mainly from a rupture of an Aneurysm, rupture of an Arteriovenous malformation or an excessively high blood pressure.
An aneurysm rupture calls for an urgent intervention to secure the aneurysm, typically within a 24 hour time window.
What is a Brain aneurysm? What are the risk factors for aneurysm rupture?
What is a Brain aneurysm? What are the risk factors for aneurysm rupture?
What is a Brain aneurysm? What are the risk factors for aneurysm rupture?

A Brain aneurysm can be best described as a balloon like out-pouching that arises from a weakened wall of an arterial blood vessel supplying the brain.
As time goes on, the weakening in the arterial wall and the hemodynamic factors that caused the aneurysm continue to making it bigger till it ruptures causing a brain bleed.
Some of the risk factors for an aneurysm rupture include smoking, high blood pressure and family history of aneurysm rupture.
When to suspect a Brain bleed ? What are its symptoms?
What is a Brain aneurysm? What are the risk factors for aneurysm rupture?
When to suspect a Brain bleed ? What are its symptoms?

An aneurysm rupture often presents with a “Worst headache of life”.
In addition to the “Worst headache of life”, other symptoms can include dizziness, weakness, sensation abnormalities, double vision, nausea, vomiting, stiffness of the neck, sensitivity to light, etc.
How can we diagnose a Brain Aneurysm?
Is an aneurysm rupture uniformly fatal? How is the recovery?
When to suspect a Brain bleed ? What are its symptoms?

A Brain aneurysm is diagnosed with a vessel imaging of the brain. A CTA or an MRA are different types of vessel imaging helpful for diagnosing an aneurysm, or arteriovenous malformation, or other vessel abnormalities.
A Diagnostic Cerebral Angiography is the gold standard test for diagnosing an aneurysm or other vessel abnormalities and in many cases its possible to treat these through the cerebral angiography route.
Do Aneurysms run in the family?
Is an aneurysm rupture uniformly fatal? How is the recovery?
Is an aneurysm rupture uniformly fatal? How is the recovery?

The incidence of familial aneurysms among SAH patients is 6% to 20%
Familial intracranial aneurysms are generally defined as the presence of two or more family members having aneurysms.
For people with family history of aneurysms an MRA can be used as a screening test.
Is an aneurysm rupture uniformly fatal? How is the recovery?
Is an aneurysm rupture uniformly fatal? How is the recovery?
Is an aneurysm rupture uniformly fatal? How is the recovery?

A scary fact about aneurysms is that many carry no symptoms until the problem is life threatening.
50% of the patients with subarachnoid hemorrhage or brain bleeding from a ruptured aneurysm do not survive.
The other 50% have a wide spectrum of recovery with going back to the life before the aneurysm rupture on one end of the spectrum to having severe disability on the other end of the spectrum.
What symptoms can unruptured aneurysms present with? When is treatment considered?
What symptoms can unruptured aneurysms present with? When is treatment considered?
What symptoms can unruptured aneurysms present with? When is treatment considered?

Sometimes unruptured aneurysms can present with symptoms from the Mass effect/volume effect due to their size and compression of the surrounding structures. In these cases elective treatments can be planned.
In case of other symptoms from what are called “sentinel bleeds”, semi emergent treatments can be planned.
Depending on the anatomy and other high risk characteristics of the aneurysm, a treatment can be planned on unruptured aneurysms. These procedures are usually controlled and well planned as opposed to the emergent procedures during an aneurysm rupture.
How are aneurysms treated?
What symptoms can unruptured aneurysms present with? When is treatment considered?
What symptoms can unruptured aneurysms present with? When is treatment considered?
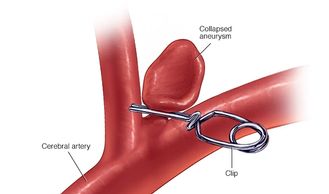
There are multiple approaches to consider for the treatment of aneurysms.
Depending on the size and location of the aneurysm, procedures may include microsurgery for clipping of the aneurysm neck, endovascular coiling, or stenting for obliteration of the aneurysm dome, or a combination of microsurgical and endovascular procedures.
Microsurgical procedures are performed by a specially trained Vascular Neurosurgeon.
Less invasive angiogram based procedures can be performed by an Interventional Neurologist, Interventional Neuroradiologist or a specially trained Neurosurgeon.
What are Interventional or Endovascular approach for treatment of aneurysms?
What symptoms can unruptured aneurysms present with? When is treatment considered?
What are Interventional or Endovascular approach for treatment of aneurysms?
Interventional or Endovascular procedures are less invasive technique for treating intracranial aneurysms that is done through a very small tube (a catheter).
The catheter is introduced through a needle puncture most often through an artery in the leg or an artery in the wrist.
The catheter can then be painlessly navigated through the arterial system until the tip of a smaller microcatheter is placed within the sac of the aneurysm for the treatment of the aneurysm.
What is Aneurysm coiling?
What are the other devices in the Endovascular repertoire?
What are Interventional or Endovascular approach for treatment of aneurysms?
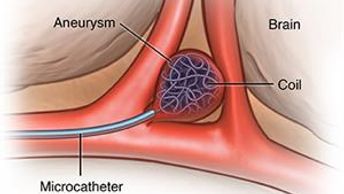
“Coils” are very soft threads of wire, usually platinum, that have a pre-specified shape when they are unsheathed from the catheter.
A series of coils are carefully placed into the aneurysm, filling the sac with the soft coils and preventing blood from flowing into the aneurysm.
Plugging the aneurysm in this way greatly reduces the chances of the aneurysm rupturing in the future.
Although aneurysm coiling is not a painful procedure, it can take several hours during which time the patient must remain very still, and for that reason these procedures are most often done under general anesthesia.
What are the other devices in the Endovascular repertoire?
What are the other devices in the Endovascular repertoire?
What are the other devices in the Endovascular repertoire?
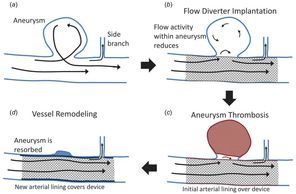
Different types of stents, including flow diverters - which divert the blood flow away from an aneurysm are also used to treat aneurysms.
A combination of devices and techniques such as stent assisted coiling is also used for aneurysms with difficult anatomy.
More recently, flow disrupters such as aneurysm web device are being used which can slow the blood flow in the aneurysm and help in treating it.
The repertoire of the devices keeps advancing very rapidly.
Is one approach better than the other?
What are the other devices in the Endovascular repertoire?
What are the other devices in the Endovascular repertoire?

For ruptured aneurysms, endovascular approach is considered better than open approach.
However, for unruptured aneurysms depending on the anatomy, location of the aneurysm and patient preference, either approach can be useful.